Brief Overview
Operation Reports may be created from the Scheduler or patient's clinical file, and are used to record the details of a patient's procedure. This includes things such as the names of any providers involved in the procedure, information about how the procedure was conducted, and any attachments of images taken in relation to the procedure. Operation Reports can only be created by Doctor users.
Short Version
- Use the Operation Report icon on the Scheduler or clinical record.
- Complete the Main Info, Details, and Files tabs as necessary.
- Click Save or Save & Print to add the report to the patient's clinical record.
Instructions
1. Click the Operation Report icon in the Scheduler or within the consult window.
A) In the Scheduler, the icon is found along the top toolbar. If you highlight a patient appointment before clicking the icon, the Operation Report will be raised for the selected patient. Alternatively, you can click the Operation Report icon without a patient highlighted to search for a patient first. ![]()
B) In the clinical file, the Operation Report icon can be found in the top right-hand corner if you are not currently within a consult.
C) If you are within a consult or quick consult, the Operation Report icon can be found in the row of icons in the top right-hand corner of the clinical window. 
2. The information loaded into the Main Info tab is populated from the Fee Estimate that was linked to the appointment.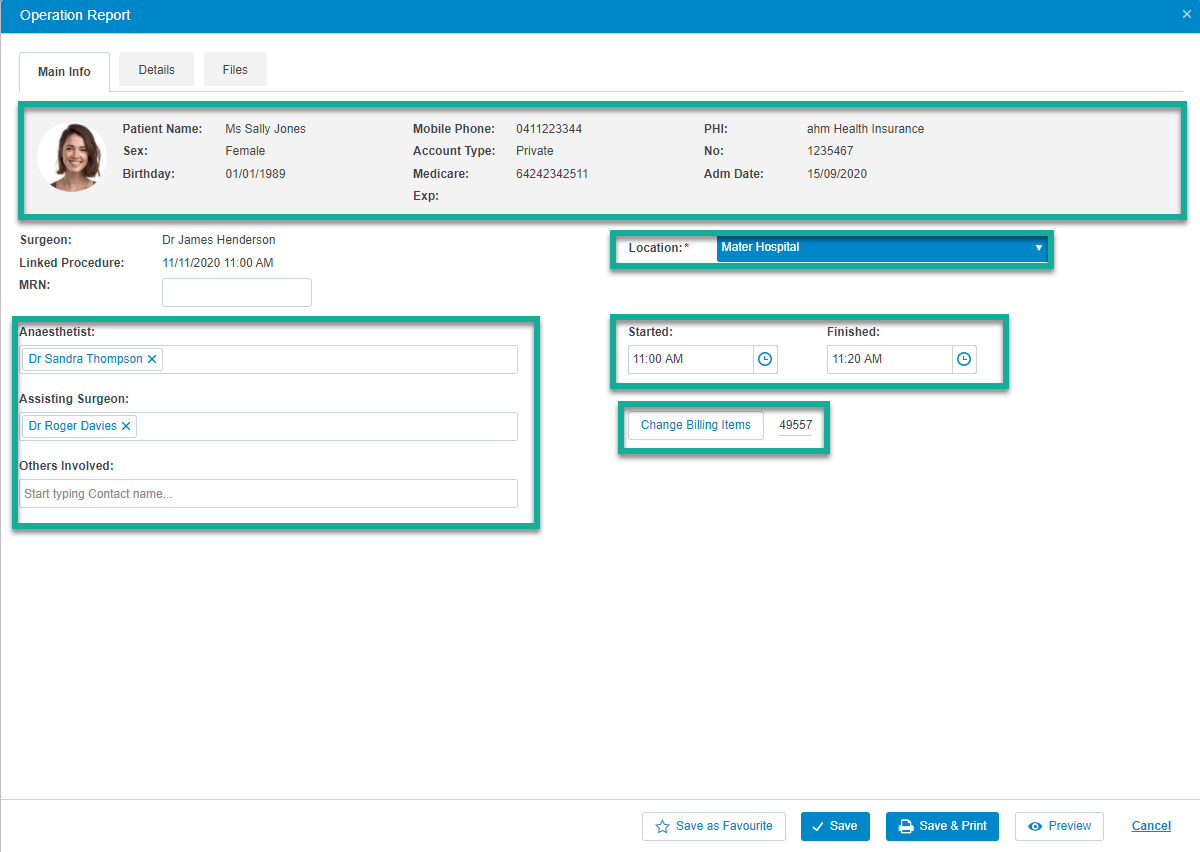
- The patient's contact information will be imported from their demographic record. If changes to these details are required, then the patient's demographic record must be adjusted before the Operation Report is created.
- The Location is imported from the linked procedure record.
- You can change an existing Anaesthetist, Assisting Surgeon, or Others Involved contact by using the x icon beside their name, and searching for a new Contact record.
- The billing items are populated from the Fee Estimate that was attached to the appointment. The billing items can be changed by clicking the Change Billing Items button, removing any incorrect items, and searching for the new items.
3. The Details tab is used to record the details about the procedure itself. This window can be templated by using the favourite and dictionary functionality, to save you from repeating similar reports.
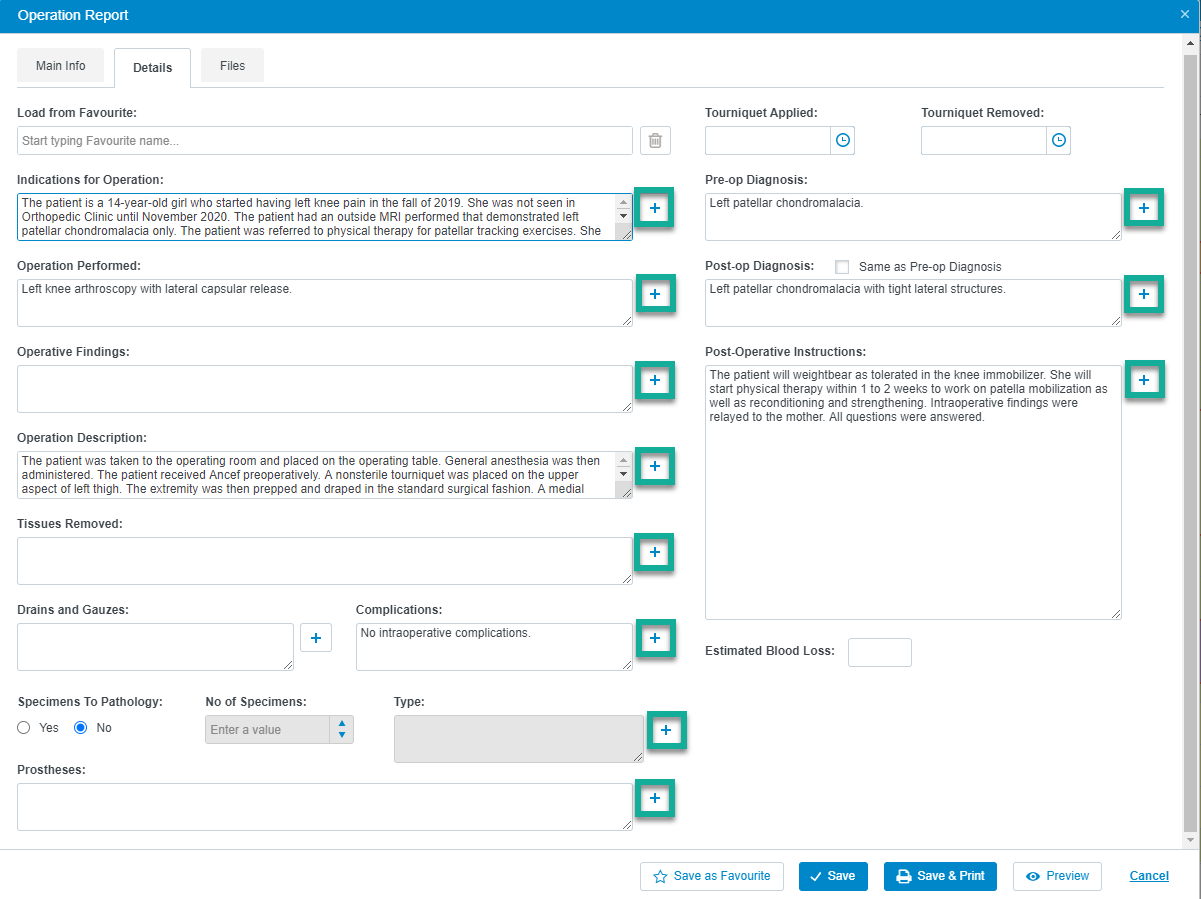
A) The Plus + icons beside each field allow you to add a dictionary item for that field. Once added, you may type only the first few letters of your dictionary item to review a list of items from your dictionary, and then press Tab or Enter on your keyboard or left click with your mouse on the suggestion, and the text will populate from your dictionary. The gif below demonstrates how to add an item to your dictionary, and how they are used to auto-populate information. 
B) After you have entered information into each field, you may save the report as a favourite, which will allow you to quickly populate an entire Operation Report in a matter of clicks. This is very useful if the information you have entered is used multiple times, or if your procedure technique is typical for a procedure of its type.
i) Once you have populated the information into the fields required, click on Save as Favourite and provide a descriptive name.

ii) You may then select the favourite from the Favourites field at the top of the window in future to populate the information. 
4. The Files tab allows you to upload an attachment to the Operation Report, which will be visible on the last page of the report.
A) Click the Add File button to open the browse window.
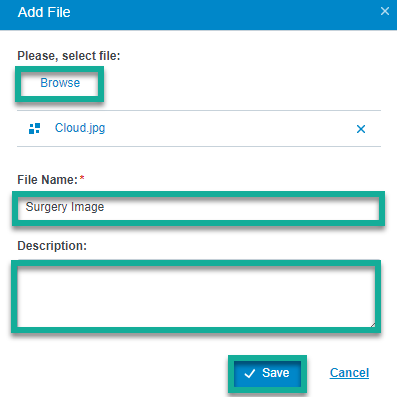
B) From here, click Browse, select the file from your computer and click Open. You may then change the File Name, and provide a Description for your attachment before you click Save.
C) The file will then be attached to the Operation Report.
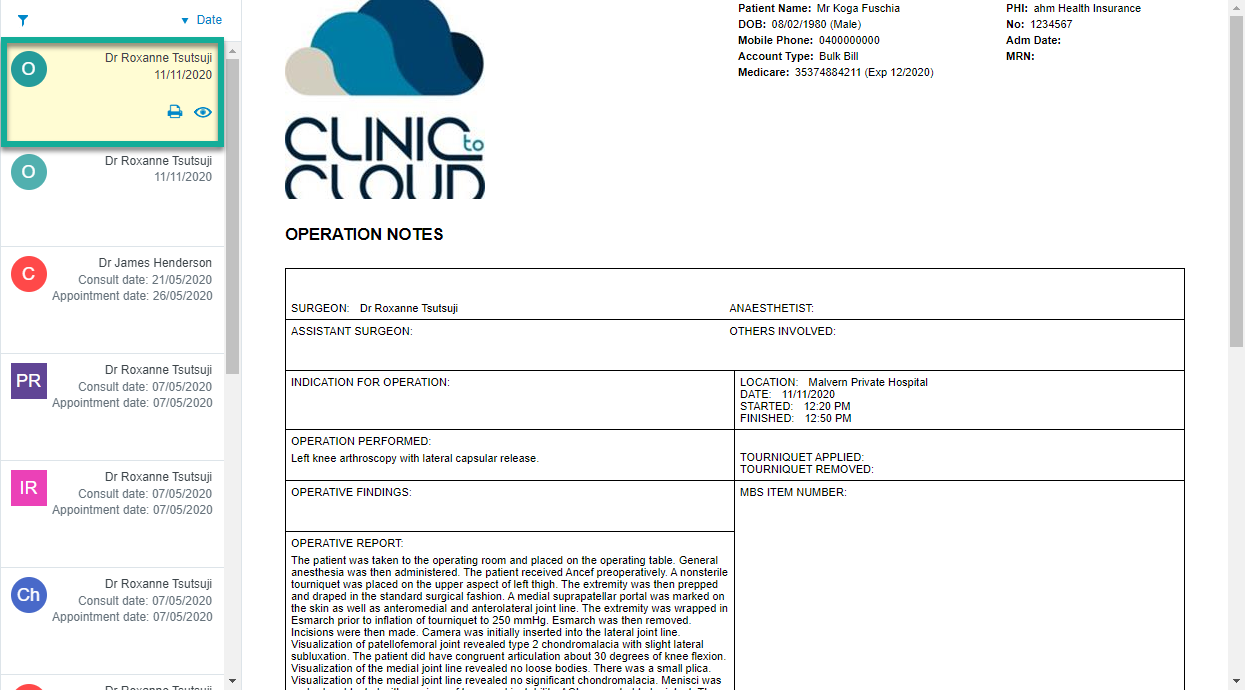
5. When you have finalised your report and added any necessary attachments, you can either click Save to save the report to the patient's record, or Save & Print to save the report and print a copy. 
6. The Operation Report will then be visible within the patient's clinical record.